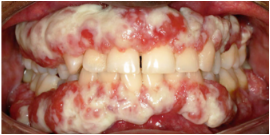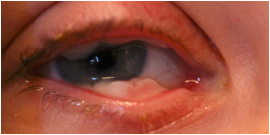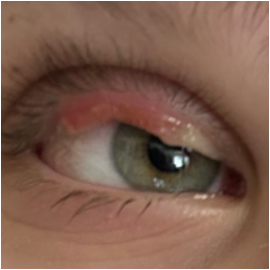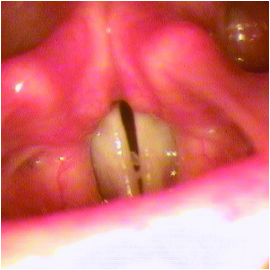



Lesions due to PLGD-1 may present in a variety of ways, from watery, stringy pseudomembranes to thick wood-like lesions. Not only does symptom severity fluctuate over time, but the overall severity of the disorder varies greatly from patient to patient depending on the location and duration of lesions. Even members of the same family impacted by PLGD-1 can present with drastically different manifestations.6
Lesions can form spontaneously, but they are typically triggered by local infection, irritation, injury, or surgical intervention.6
Explore Image Gallery >